Introducing Food Allergens to Baby
When should you introduce food allergens? It's probably earlier than you thought! Learn how to safely introduce cow’s milk, egg, peanut, and other common food allergens.

Key Points
Introduce early and serve often
The evidence is clear: food allergies can be prevented by introducing common allergens like peanut and egg in infancy and regularly serving them, especially for babies with an increased risk of food allergy.
Introduction can usually begin at home
Most babies can begin allergen introduction as soon as they are ready to start solids around 6 months of age. However, you may decide to start earlier (around 4 months of age) if your baby has eczema or an existing food allergy.
Consistent exposure over time is key
Once a food allergen has been introduced, you need to regularly offer it (ideally twice a week) to lower the chances of your baby developing an allergy to that food.
Why Doctors Recommend Starting Early
In the United States, food allergies in children rose an astounding 50% from 1997 to 2011 and the prevalence of peanut and tree nut allergies tripled during this time.[1] Interestingly, this is roughly the same period of time in which parents were advised to refrain from introducing peanuts and other allergens until well beyond the first birthday.[2]
That began to change after 2015, when a groundbreaking study demonstrated how the early introduction of peanuts to at-risk babies could reduce the risk of developing peanut allergy by as much as 81%. In other words, delaying peanut introduction could actually increase the likelihood of peanut allergies developing.[3]This landmark study led medical professionals to revise their recommendations around the introduction of peanut and extrapolate the study’s findings to other food allergens like egg, cow’s milk, and wheat. Allergists and other medical professionals now recommend introducing many common food allergens well before a baby’s first birthday.[4]
This shift in guidance may have helped turn the tide. In recent years, food allergies to peanut have dramatically decreased among children in the United States. In 2025, a major study confirmed the link between recommendations for early allergen introduction and a significant decrease in food allergies in babies and toddlers at risk of developing food allergies.[5] Our hope is that food allergies will continue to decline as more families take advantage of the preventative benefits of introducing allergens early and regularly serving them.
Top Allergens for Babies
Although it is possible to be allergic to any food, the most common food allergens in the United States are those listed below.[6] Learn more about common food allergens around the world.
Common Allergens for Babies
Allergen | Foods to Introduce Allergen to Baby | Safety Tip |
|---|---|---|
Cow's Milk | yogurt or soft cheese like ricotta | pasteurized |
Egg | hard-boiled or scrambled egg (yolk and white) | well-cooked, mash into tiny pieces |
Finned Fish | low-mercury fish (cod, salmon, sardines, trout) | fully cooked and flaked (no bones, but skin is okay) |
Peanut | peanut butter | honey-free, smooth texture, thin with water until saucy (no clumps) |
Sesame | tahini or ground-up sesame seeds | if thick, thin with water |
Shellfish (Crustacean) | shrimp, crab, crayfish, or lobster | fully cooked and finely chopped (no shells) |
Soy | tofu or soy yogurt | mash tofu |
Tree Nuts | nut butter or ground nut sprinkle | honey-free, thin with water until loose and saucy |
Wheat | wheat cereal or breadcrumbs | cook cereal with water, use sesame-free breadcrumbs |
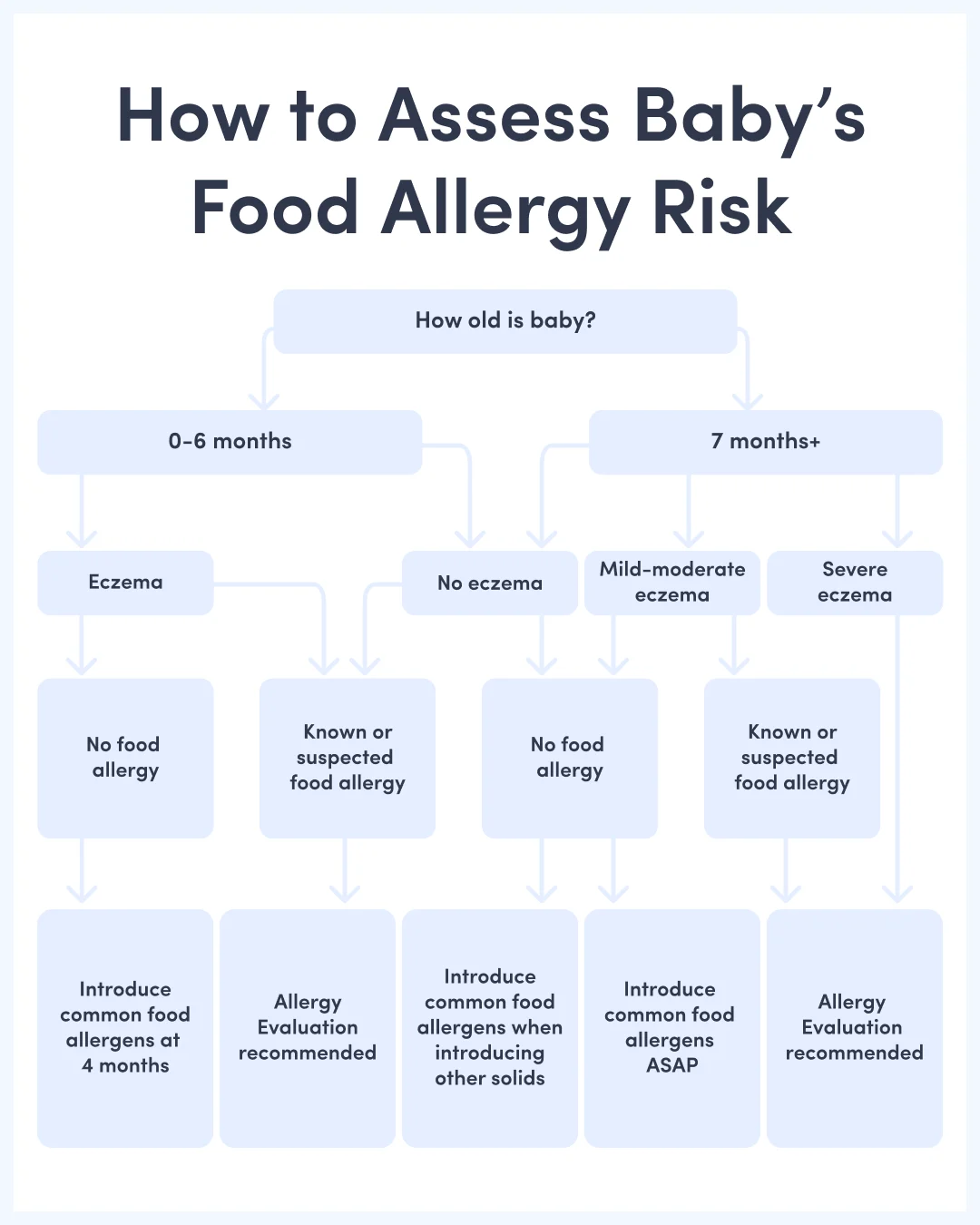
How to Assess Baby's Food Allergy Risk
Step by Step | Why It Matters |
|---|---|
Step 1: Start with their age | Babies around 6 months of age can benefit from allergen introduction within a week or so of starting solids, and for some babies, introduction may be recommended even earlier if they face an increased risk of food allergy. Delaying introduction to allergens can increase the risk of allergies developing, especially if baby has eczema. |
Step 2: Check for eczema | Babies with eczema of any severity are more likely to develop food allergies, but that is not a reason to delay introduction to common food allergens. Babies with eczema can still reap the protective benefits of introducing allergens, and are most likely to benefit from early introduction. |
Step 3: Evaluate allergies | Babies with a known or suspected food allergy to a food are more likely to develop allergies to other foods. For these babies, an allergy evaluation is recommended before introducing other allergens at home (especially if the original reaction was severe). |
Step 4: Take action | The risk of food allergy is high in babies with eczema and/or pre-existing food allergy, so talk to your doctor and make a plan to introduce allergens as soon as possible. If the risk is low, allergen introduction should begin at home as soon as they are ready to start solids (usually ~6 months). |
Babies with eczema and/or a known or suspected food allergy face an increased risk of developing food allergies. For many of these babies, introduction at the early age of 4 months—done safely—can significantly reduce the chance of developing a food allergy. Check out tips for introducing allergens before 6 months of age.
Signs That Do NOT Increase Risk
These factors alone do not place a baby at a significantly higher risk for food allergy.
Being breastfed vs. formula-fed
Having reflux, colic, or gas
Having a sensitive stomach
Being born prematurely (by itself)
Parent has food sensitivity (not an allergy)
For Babies with Increased Risk of Food Allergy
Next Steps | Why It Matters |
|---|---|
Talk to your doctor | Your doctor may recommend introducing peanut, egg, and possibly other common allergens before the child is developmentally ready to start solids. Older babies (7 months of age and up) with severe eczema or an existing allergy to a food may have already developed food allergy, and it is especially important to consult your doctor before you get started. |
Start early | Introduce common foods like peanut and egg earlier rather than later, ideally around 4 months of age. Delaying introduction will NOT prevent food allergies from developing. |
Start small | Allergic reactions can be more severe when more of the allergenic food is consumed. Start with a small amount (such as 1/4 teaspoon) and gradually work up to larger quantities if there are no symptoms of an allergic reaction. |
How to Introduce Food Allergens to Babies
Introducing food allergens doesn’t have to be scary. You can start with a very small amount of the allergen to minimize any possible reaction and slowly work up to larger servings.
1. Assess the risk
Check out How to Assess Food Allergy Risk to determine the risk. If the risk is low, proceed with allergen introduction at home.
2. Be prepared
Review the symptoms of an allergic reaction before you begin. While an allergic reaction is unlikely, it’s best to know what one looks like just in case.
3. Choose a day to start
Pick a day when you are able to closely observe your baby. The introduction can take place over the course of one day (at breakfast, lunch, and dinner, for example) or on consecutive days.
4. Choose a food
Choose one common food allergen to get started. We recommend starting with peanut or egg because the evidence for the protective benefits of early allergen introduction is strongest with these common food allergens.[7]
5. Go one at a time
Complete one allergen introduction before beginning the introduction of another. This way, if there is a reaction, you’ll know which food was responsible.
6. Prepare the food
Start with a small quantity (the smaller the quantity of allergen ingested, the less severe an allergic reaction may be) and gradually work up to offering more.
7. Start early in the day
Start at breakfast or right after a morning nap. This way, it may be easier to contact your doctor for guidance in the unlikely event of a reaction. Most reactions occur shortly after exposure, which is why it is best to introduce allergens when at least one adult can focus their full attention on baby, ideally for at least two hours and without distraction from other children or activities.
8. Start with a small taste
Scoop a small amount with the tip of a spoon or your finger, then hold it near their face, and wait for a moment to let them observe the food. They may lean in with their mouth and try to taste—let them. If they do not budge, slowly move it a little closer to their face, then pause and give them another opportunity.
If they hesitate, but otherwise seem engaged, you can gently touch the spoon, teether, or finger to their mouth or tongue, but don’t force it. You want baby to associate food with positive experiences, and forcing food into baby’s mouth does not help achieve this goal. If they are not actively engaged, turn their head, or push the spoon, teether, or finger away, they are communicating to you that they want to stop. Take a break or end the meal. You can always start again later.
Once they’ve tried their first taste, offer more tastes until you’ve offered all of the food you’ve prepared, or they are showing signs that they’re done… whichever comes first. It’s okay if they do not consume all of the food you’ve prepared. Just a small taste is enough to get the introduction process started.
9. Watch for signs of an allergic reaction
After baby has a small taste, move on to your next activity while observing baby. Ideally keep baby in just a diaper or periodically check the skin on their stomach, chest, and back for any signs of rash or redness. If baby shows no signs of a reaction after 15 minutes, proceed with your day (but stay alert). Most reactions occur within minutes (but up to 2 hours) after exposure.
If there are no symptoms of an allergic reaction after a couple of hours, offer the allergen again, and repeat the steps above. A baby may not have an allergic reaction the first time they are exposed to the food, so be watchful as you gradually increase the quantity served. The allergen introduction is complete after the third serving.
10. Aim for regular exposure
Once an allergen is introduced, serve it at least once a week, and ideally 2 to 3 times a week until at least 6 years of age. It’s okay if you need to take a break when your baby is sick or you are traveling. The goal is to offer food allergens frequently when possible to help your child reap the full preventative benefits of early allergen introduction.
If Baby Has an Allergic Reaction: What Comes Next
If baby had an allergic reaction, you may feel scared and unsure of what to do. Here are the most important next steps after the reaction is treated.
▶ Consult an allergist — even if you think you know what caused the reaction
An allergy evaluation is far more than a test. At the visit, your allergist will review baby's history, confirm a diagnosis, and prescribe emergency medication. You will also learn how to use an epinephrine auto-injector (like an EpiPen) and get a written food allergy action plan. These tools will help you keep your baby safe, and they are worth the wait for an appointment.
▶ Learn what allergy testing can and cannot tell you
There are two common tests used to check for food allergies: a skin prick test and a blood test. Both tests are good at identifying allergies, but neither one is perfect. False positives are common, especially with blood tests. Neither test can tell you how bad a future reaction might be. Your allergist will always review the test results together with baby's history—not just look at the test results alone.
▶ Do not offer the suspected allergen while you wait
Unless your doctor advises you otherwise, it is safest to avoid offering the food that you think triggered an allergic reaction while you wait for an appointment with your allergist. Reactions can be hard to predict, and if baby is truly allergic, the next reaction could be worse than the first. You don’t want to be unprepared.
▶ Don’t ask for allergy testing on foods baby has never reacted to
Testing too many foods at once can result in false positives. It can also create gaps in baby’s diet when you avoid offering foods that were never actually a problem. Targeted testing, guided by your baby's specific history, is the right approach.
▶ Get a food allergy action plan and epinephrine training—and review often
You should leave the appointment with your allergist with a written food allergy action plan and hands-on training with an epinephrine auto-injector (like an EpiPen). Share the plan with everyone who cares for baby and make sure they know what to do if baby accidentally eats the wrong food. Practice with your EpiPen trainer a few times a year so the steps feel natural before you ever need them.
▶ Know that many food allergies are outgrown
Allergies to egg, milk, soy, and wheat often go away on their own during childhood. Allergies to peanut, tree nuts, sesame, and seafood tend to stick around, but some children do outgrow them. As baby grows, your allergist can check whether the allergy is still there using skin tests, blood tests, and supervised food challenges.
▶ Treatments are improving, and there is real reason for hope
Food allergy care has come a long way beyond just avoiding problem foods. There are now treatments that can help the body get used to an allergen over time.
Two common treatments are oral immunotherapy and sublingual immunotherapy. Both work by giving the body tiny amounts of the allergen, slowly increasing the dose until the body becomes less sensitive. Research suggests that starting these treatments early in infancy or toddlerhood may work better than starting later. These treatments must always be done with an experienced allergist, never at home.
One newer treatment is Omalizumab (Xolair). It is a medicine that can help children as young as 12 months with an IgE-mediated food allergy tolerate more of an allergen and lower the chance of a bad reaction if they accidentally eat it. Other new treatments are also becoming available or in development, including allergy medicines that come as a nasal spray or a film that dissolves under the tongue.
When can I reintroduce the allergen?
Don’t reintroduce a known or suspected food allergen on your own. Consult your allergist to come up with a plan before you offer the food again. Your allergist can help confirm the diagnosis and determine a safe and appropriate time to re-introduce the allergen. This may need to be done slowly in the clinic, while baby is monitored by healthcare professionals who are trained to rapidly manage allergic reactions. This is called an oral food challenge.
Do I need to avoid other common food allergens?
No. Just because baby reacted to one food allergen, it doesn’t mean that all common allergens need to be avoided. It’s actually important to keep giving baby any common food allergens that have already been successfully introduced. The science also shows that you don’t need to stop introducing new allergens either.
How long should I wait before introducing another common food allergen?
As long as baby’s original food allergy reaction has resolved, you can continue other common food allergens, sometimes as soon as the next day. However, if baby’s still not back to baseline, it’s a good idea to wait so any symptoms can clearly be linked to the new food.
I'm so scared to keep feeding. How to move past the fear?
It’s totally understandable to feel anxious after baby experiences an allergic reaction. Trust that, with the help of your doctors, you can create a plan for baby to safely introduce new foods while still avoiding known allergens.
Remember, introducing allergens is the best way to prevent food allergy, and babies who delay introduction are more likely to develop additional allergies. If the fear of a reaction is truly paralyzing, consider seeking support from a food allergy-informed counselor or therapist. They can help you work past the anxiety. You can also talk to your allergist, who may be able to offer oral challenges in the clinic.
Food Allergies Around the World
The United Nations and World Health Organization have established the Codex Alimentarius (Codex), a set of international food standards, guidelines, and codes of practice designed to ensure the safety of the global food supply.
The Codex guidelines recommend disclosure of the following food allergens:
Egg
Milk
Fish
Crustaceans
Gluten
Soy
Peanut
Tree nuts
Sulfites (at concentrations 10 mg/kg or more)[8]
These foods comprise the majority of food-induced allergic reactions in most areas of the world. However, common food allergens vary worldwide and are influenced by genetics, the foods most consumed in those regions, and cross-reactivity with airborne allergens, among other factors.[9] [10]
Africa
Several African nations, including Egypt, Malawi, Morocco, and South Africa, have common food allergen lists that mirror that of the U.N./WHO Codex.
Recent research suggests that food allergies may be underdiagnosed across the African continent.[11]
Asia
There is no central regulatory body governing food allergy labeling for the Asian continent, and common food allergens vary in different areas.
Common food allergen lists for China, Hong Kong, Singapore, Thailand, and Vietnam are similar to the U.N./WHO Codex.
Common food allergens in Japan and South Korea include allergens outlined in the UN/WHO Codex, as well as buckwheat.
Additionally, South Korea lists chicken, beef, pork, pine nuts, peach, and tomato as common food allergens.[12]
While chickpeas are not designated as a common allergen requiring labeling, chickpea is a significant emerging food allergen in India.[13]
Europe
The European Union (EU), UK, and EEA (Iceland, Liechtenstein, Norway) recognize 14 common food allergens/intolerances—gluten-containing cereals, egg, milk, soy, peanut, tree nuts, fish, crustaceans, mollusks, celery, mustard, sesame, lupin, and sulfites.
Non-EU countries in the region also follow similar guidelines, with minor variations from country to country.
Latin America & Caribbean States
CARICOM (an organization of Caribbean states), the Central American Technical Regulation countries, Brazil, Venezuela, Argentina, and Chile recognize the same common allergens as outlined by the UN/WHO Codex.
North America
In the United States, there are currently nine foods required for labeling as major food allergens—milk, eggs, peanuts, tree nuts, fish, sesame, shellfish, soy, and wheat.
Mexico and Canada recognize and require the labeling of allergens as outlined by the UN/WHO Codex.
Canada includes mustard and sesame on its list of top allergens.
Southwest Asia
The Gulf States Organization (GSO) recognizes the following allergens—gluten-containing cereals, egg, milk, soy, peanut, tree nuts, fish, crustaceans, mollusks, celery, mustard, sesame, lupin, and sulfites.
Of note, sesame is a very prevalent allergen in this region, and in Israel, studies have identified sesame as the second most common food allergen in children, after milk.
Southwest Pacific
Australia and New Zealand require labeling for common allergens as outlined by the UN/WHO Codex.
Additionally, Australia and New Zealand require labeling for lupin, sesame, bee pollen, and royal jelly.
Frequently Asked Questions
Not unless advised by your doctor. You should introduce common food allergens, especially egg and peanut, as soon as your baby is ready to start solids, or earlier if your baby has an increased risk of food allergy. Delaying introduction can actually increase the risk of food allergies developing.
Although food allergies can run in families, family history alone is not a reason to delay allergen introduction. On the contrary, early introduction remains protective for most babies—especially those with allergic parents or siblings. Allergy specialists advise that siblings of children with food allergies and children of parents with food allergies can generally introduce common food allergens at home without any pre-screening by an allergist if they are not at higher risk due to severe eczema or another pre-existing food allergy.
Start with peanut, egg, or cow’s milk. You do not need to follow a prescribed order of allergens, but you should prioritize these allergens because they are the most common food allergens in babies and they are staple foods across different cultures. Aim to introduce at least one of these foods every few days, ideally starting by the second or third week of starting solids. Once you’ve introduced peanut, egg, and cow’s milk, proceed with introducing other common food allergens that align with your family’s dietary preferences.
Although some food protein does pass to baby through breast milk, this is not a reliable way to introduce or maintain exposure to common food allergens, and so doesn't "count" as early introduction.
We recommend starting tree nut introduction by choosing a nut that is one of the most common triggers of food allergies in babies and toddlers: almond, cashew, hazelnut, and walnut. Introducing each of these nuts individually and serving them regularly will help prevent food allergies to cross-reactive tree nuts. For example, if cashew is well-tolerated, pistachio can be offered to baby without a formal introduction. Same goes for walnut and pecan.
There are many varieties of tree nuts, and once the major tree nuts (almond, cashew, hazelnut, and walnut) are introduced, you may also choose to separately introduce other tree nuts, such as Brazil nut, pine nut, or macadamia nut, but you do not need to introduce every single one. Focus on introducing tree nuts that are common in your diet, and regularly offer them to help prevent food allergies from developing, ideally twice a week. Once tree nuts are successfully introduced, they can be served together. Families often choose to keep up exposure to tree nuts with mixed nut butter.
No. It is possible to be allergic to one tree nut but not others. Introducing tree nuts separately lets you rule out food allergy to one variety before introducing a different one. Once all tree nuts in mixed nut butter have been introduced separately, it is a great way to keep up exposure to allergens.
Yes, as long as the well-tolerated allergen has been regularly served (ideally twice a week) since it was introduced. If the well-tolerated allergen has not been served in the last two weeks, you’ll want to reintroduce it first. In the meantime, we recommend introducing the new allergen on its own or alongside another food that baby has been regularly eating.
If your baby doesn’t consume the entire serving of allergen offered when you offer it, that’s okay. Relatively modest quantities of allergen exposure (~2 grams of allergen protein per week) can be effective for allergy prevention, as long as it is regularly offered over time.
No. You don’t need to wait 3 to 5 days between introducing new foods. That said, you should introduce only one common allergen at a time. It is perfectly fine to introduce an allergen with other new foods baby has not tried, though for ease, many parents prefer serving a new allergen on its own or only alongside foods baby has already safely eaten.
Waiting a few days before introducing each new food can significantly limit the timely introduction of different tastes and textures, and potentially increase the risk of food allergy in the future. In general, the benefits of introducing a variety of new foods outweigh the risks of a potential reaction or sensitivity.
No. It is not necessary (and it is generally not cost-effective) to rely on powders or medicalized food products when introducing food allergens or keeping them in the diet. A food allergen may be introduced by safely preparing it in a way that meets baby’s age and developmental ability, and you can look up any food in our First Foods® database to see how it’s done. However, it's important to do what works for your family. Butters, powders, and puffs can help with allergen introduction or maintenance when there is limited access to food (while traveling, for example), or if baby has a medical condition that interferes with the introduction of solid food.
Review the full list of allergy symptoms in babies before you get started. Most babies will never experience an allergic reaction, but it can happen—and it is important to understand how to spot an allergic reaction and how to take action if it happens.
Not usually. Acidic foods like berries, citrus, pineapple, and tomato often cause a harmless rash on the skin that comes into contact with the juices, typically around the mouth and chin.[14] Contact rashes usually dissipate with a gentle cleanse after mealtime. Pat with a wet washcloth; don’t rub to avoid further irritating the skin. To help protect the skin from contact rashes, you can apply a barrier ointment (pure petroleum jelly or a plant-based oil and wax combination) to the face before mealtime.
If the rash is widespread (such as all over the torso, arms, and legs), it is more likely to be an allergic reaction than a contact rash and you should seek immediate medical guidance. Check out Allergy Symptoms in Babies to learn more.
Talk to your doctor. They can help sort out whether symptoms are more consistent with a true food allergy, a food intolerance, or a temporary reaction related to illness, eczema, or feeding stage. This step matters. Unnecessary elimination of food from your child’s diet can sometimes increase the risk of an allergy developing, rather than reduce it.
After you connect with your doctor, they will likely attempt to confirm or rule out a food allergy. No single test tells the whole story—the history matters most. They will need to know what foods they’ve eaten, including what foods you believe caused the reaction, as well as when allergy symptoms appeared.
If a food allergy is confirmed, your doctor can advise you on how to safely feed your child while avoiding food allergens. They can also prescribe emergency medication and review an action plan for how to treat reactions and eventually reintroduce the food when it is safe to do so. Food allergies often fade over time, and in some cases, early and careful management—under medical guidance—can improve the chances of developing long-lasting tolerance.
Consult your doctor before attempting to reintroduce any food that has triggered an allergic reaction in your child. If baby has experienced an allergic reaction to a food, do not offer the food again until you can make a plan with licensed professionals, ideally a pediatric allergist. Allergic reactions can be unpredictable, and a child who experienced only a mild reaction at first might experience a more severe reaction later on. Your medical team can guide you on how best to proceed, and they may recommend reintroduction under medical supervision. This way, baby can be monitored and immediately treated if an allergic reaction occurs.
IgE-mediated allergies are what most people think of when they think of a food allergy. They result in symptoms very quickly after allergen ingestion, often within minutes. IgE-mediated allergies are diagnosed by confirming a clinical history of reactivity with a positive blood test or skin prick test at the allergist’s office. Several IgE-mediated food allergies (such as cow’s milk, egg, soy, and wheat) are commonly outgrown in early childhood.
Non-IgE-mediated food allergies are immune hypersensitivities that do not involve the production of IgE antibodies. Instead, other parts of the immune system, such as white blood cells, are activated. Symptoms typically take longer to appear than IgE-mediated allergies (from a few hours to days after eating) and they show up in various ways, including skin rashes and gastrointestinal symptoms.
There is no standardized testing available for non-IgE-mediated food allergies, so the diagnosis is based on clinical history. The recommended treatment? Avoid the allergen and reassess at regular intervals to determine if the allergy has been outgrown. Epinephrine and antihistamines will not treat symptoms of non-IgE-mediated food allergy. However, in certain cases, anti-nausea medication, steroids, and biologics may be used to counteract the bothersome symptoms and inflammatory response. Check out FPIES & Babies for more information about one type of non-IgE-mediated food allergy.
Fortunately, allergies and Oral Allergy Syndrome (OAS) are not passed along to baby through breast milk. Concerns about potential food allergies should not discourage parents from offering breast milk, especially since breast milk offers a variety of nutritional and immune-supporting benefits for baby. [15] Avoiding common food allergens either during pregnancy or when lactating hasn’t been shown to prevent food allergies.[15]
Rest assured that you are unlikely to experience a serious allergic reaction from simply being in the vicinity of your allergen or even from handling it. Most patients with food allergies react only upon ingestion. That said, there are steps you can take to minimize your risk of a reaction.
Before mealtime: Avoid prolonged skin contact with the allergen. If you cannot wash your hands promptly afterward, wear gloves. If you are breastfeeding baby, consider offering a breastfeed just prior to the meal to avoid the need to nurse immediately after (allows time for the allergen to clear baby’s mouth/saliva).
At the table: If you have a carpet or rug, place the high chair over a splat mat or move the high chair to a non-carpeted surface. You could also consider feeding baby outside. This is also a great time for disposable placemats, plates, and utensils.
During introduction: Offer the allergen at the beginning of the meal and immediately follow up with another food to which neither you nor baby are allergic. This will reduce the allergen content in baby’s saliva.
After mealtime: Clean their hands and face thoroughly, wipe down the eating surface and chair, and remove their clothing so it can be washed. Consider waiting a few hours and offering baby a few sips of water or gently brushing baby’s teeth and gums to clear out any remaining allergen residue prior to breastfeeding baby after the meal, as trace amounts of baby’s saliva can backflow into the nipple while nursing.
Lastly, try to stay calm, even if you are nervous at first. Children pick up on the feelings of the adults around them. With practice, offering your allergen to baby will get easier and become routine. If you feel very nervous, this is an excellent opportunity for a non-allergic parent, caregiver, relative, or friend to spend quality time with baby.
It depends. Cheese and yogurt contain the same allergenic proteins as cow’s milk, and they can trigger allergic reactions in sensitive babies.[16] However, if a baby is not highly sensitive to casein (the heat-stable protein in milk), they may be able to tolerate cow’s milk, cheese, or yogurt fully baked in a biscuit, cake, or muffin. Some babies can also tolerate less extensively heated cow’s milk, cheese, or yogurt in fritters, pancakes, or waffles. However, this should be discussed with your healthcare professional before attempting it in the home setting. Check out Cow’s Milk for Babies & Toddlers to learn more.



